Vestibular Migraine
Through our experience, we have daily observed some patients who presented a previous diagnose of Menière Disease.
The Neurootological Anamnesis highly denotes in these patients, not only the traditional trilogy –vertigo, tinnitus, hypoacousia-, but being it very frequently joined to some other symptoms, such as headache or migraine.
The combination of vertigo and migraine indicates the possibility of being in the presence of a central pathology of vascular etiology.
From the 7800 patients selected from our Data Bank, 24% belong to vertigo group, 54% to vertigo-migraine group and 22% to migraine group.
As first and main step, it should be avoided any confusion in diagnosis and therapy, i.e. treating every patient presenting the very well known Menière trilogy as a simple lesion of the inner ear, without taking into account that the equilibrium system is something more complicated than a semicircular canal, where it does not only exist a ear and an auditive nerve, disregarding organs and most important vias as: brainstem, cerebelum, thalamus-cortical projection via, cerebelum-oculomotor via, cortical and cognitive vestibular areas, etc.
Any alteration in the circulatory haemodynamics and in neurotransmission in this complex of nucleus and vias will produce a Menière-like Syndrome, together with or without any other symptoms.
At last, a proper diagnosis of these affections enables us to establish a proper therapy towards three directions:
- Symptomatological
Directed to counteract sharp pain symptoms.
- Etiopathogenetic
Directed to the type of vascular or neuronal affection.
Improving
- Cerebral circulation
- Active transportation of substances through haematoencephalic barrier (artery / brain)
- Neuronal metabolism
- Topodiagnostic
Which also makes it possible to establish a therapy in order to prevent future irreversible cerebral damages, as it happens in cerebrovascular diseases.
Advances in basic research in neurosciences and the introduction of new non-invasive techniques, that make possible the detection of weak signals of the brain, improving diagnosis and treatment of the Vestibular Migraine
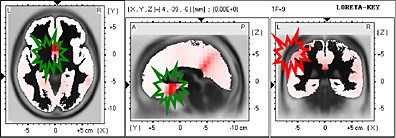
We use at our laboratory –Otoohtalmological Neurophysiology, Buenos Aires, Argentina Dr. med. G. Bertora and Dr. med. J. Bergmann– the EEG register in 21 derivation channels. The use of a specialized software Low Resolution Brain Electric Tomography – LORETA-. (Pascual-Marquí et al., 1994) makes possible obtaining functional imaging of the brain in 2D and 3D.
A comparative study using Low Resolution Brain Electric Tomography (LORETA) in 120 patients who have consulted on vertigo and migraine and the results were compared vs. 390 patients from our Data Bank. (J. Bergmann, G. Bertora – 2004).
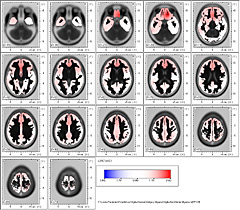
The Brain Electric Activity Mapping in the patients consulting on vertigo and dizziness joined to migraine presents in Delta Band in 2.25 Hz frequency, a combined form between the group of patients with Menière Disease and migraine exclusively. Dipoles are placed in Brodmann areas 25 and 31.
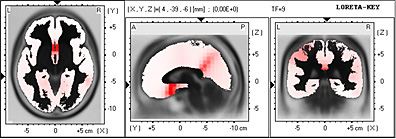
These areas bilaterally comprise the Medial Frontal Gyrus and the Parietal Lobe with left prevalence.
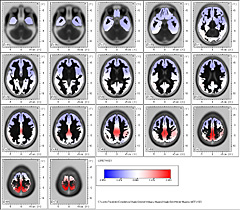
En los 5 Hz de frecuencia correspondiente a la Banda Theta se observa una importante frontalización comprometiendo las áreas de Brodmann 25 y 24.

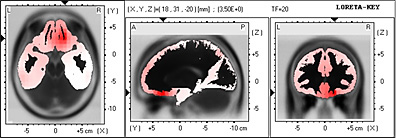
These Brodmann areas are located in the Medial Frontal Gyrus and in the Limbic Lobe and Anterior Cingulate with left prevalence.
Finalmente en la Banda ßeta2 en la frecuencia de 19.50 Hz se observa el dipolo ubicado en las áreas de Brodmann 7 y 3.

In ßeta 2 Band in 19.50 Hz frequency, the dipole is observed placed in Brodmann areas 7 and 3.
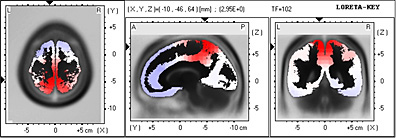
These areas comprise both Parietal lobe.

Summing up
The vestibular migraine has an important cortical representation in:
- Parietal lobe and Frontal lobe (Brodmann 25) – Delta Band
- Parietal lobe right and left – ßeta Band
- Medial Frontal Gyrus, and in the Limbic lobe and Anterior Cingulate –Theta Band
Study of the temporal distribution which the brain electrical tomography makes possible, opens a new field in Vertigo and Migraine.
The Vertigo Syndromes together with migraine are typical signs of vestibular headaches, affecting the temporo-parietal junction and the prefrontal areas.
The regular Menière Syndrome (vertigo-hypoacusis-tinnitus) has an important cortical representation in frontal areas Brodmann 25, Limbic Lobe and the Parahippocampal Gyrus.
Through our work published in 2001 Vertigo and Migraine using as a study method the Brain Electrical Activity Mapping, we have met the following conclusions:
In Brain Electrical Activity Mapping, we observe a disorder of the electrical activity in paracentral areas C3 and C4 in patients with vertigo-migraine but not in the vertigo group of patients.
But through the brain electrical activity mapping it is only possible to observe some superficial variations in cerebral electrical activity.
It is as observing the earth from a satellite and try to guess what is going on under the surface. Through LORETA, it is not only possible to study spatial distribution but also knowing the different cerebral activity areas in deep zones.
The frontalization present in all these patients and the involvement of the limbic lobe and prefrontal lobe is extensively demonstrated in Menière or Vestibular Migraine ( Migraine and Menière Syndrome).
Our research and publications
Brain Electric Tomography – LORETA
- Archives for Sensology and Neurootology in Science and Practice. ASN
Volume 2 - 2004
Menière Syndrome and Vestibular Migraine: Cortical Brain Projections
Dr.med. Guillermo O. Bertora, Dr.med. Julia M. Bergmann (Buenos Aires - Argentina)